




Several years ago, I went to consult on an 11-year-old Hmong child who suffered from cirrhosis due to vertically transmitted hepatitis B.
The child looked sick, jaundiced and with a protuberant abdomen from ascites - however, he was alert and engaged during the visit. His preoccupied father –who did not speak English at all-sat on his haunches in a corner of the room. The family spoke an uncommon dialect in the Hmong language, and that day, we could not find an interpreter, so the child had to take on the role of patient, translator, and respectful son. The resilience of children never ceases to amaze me! Choosing my words carefully, I told the child that his liver was sick and that he needed a liver transplant. I described the process of the evaluation, the transplant operation and so forth, and he relayed the information to his dad in their own language.
A few days later, I was informed that the father refused the transplant. However, the social worker pointed out that the reason for his refusal was not around the transplant itself, but a cultural barrier between the Hmong and the Western cultures. She suggested that I needed to go back and address the father and not the child, even if the father didn’t understand a word of English. This time we also had the help of an interpreter. So, I did. A day later, the father agreed to the liver transplant.
As I watch the daily news of families and children being displaced all over the world because of wars, natural disasters, running away from poverty or crime, I think of my experience with the Hmong family many years ago. As healthcare providers and members of an international organization, we need to recognize that a treatment plan must meet the patients' social, cultural, and linguistic needs. After all, cultural competency is essential for improving survival and quality of life in transplantation.
Please read on to be updated on important ongoing initiatives within IPTA. I look forward to seeing you in Prague!!
Carlos O. Esquivel
IPTA President
Allied Health & Nursing Professionals Committee

The Allied Health and Nursing Professional Committee is a vibrant group of members from a diverse background including Nursing, Pharmacy, Dietetics, Rehabilitation and Psychology, with representation from across the globe, including North America, Africa, and Europe. We meet bi-monthly and have been focusing on several initiatives, including the following highlights:
- International Allied Health and Nursing Professional Practice Survey:
Goal of survey: To describe the prevalence, diversity and clinical practice focus of AHNP team members within each centre globally. This information will serve as a foundation to help inform and develop a greater understanding of multidisciplinary team composition, and framework regarding professional practice. We are hopeful that by better describing the varying professional practices of our colleagues, we will be able to understand the extremely valuable role that Allied Health and Nursing play in improving pediatric transplant outcomes, tailor our ongoing educational endeavors to be of greater relevance, and hopefully encourage growth in our Allied Health and Nursing IPTA membership.
Implementation: Following the completion of a pilot study, several iterations were made before finalizing survey to include questions related to participant demographics, centre transplant practices, funding, scope of practice, and COVID-19 related practice issues. The survey was developed using REDCap and distributed (Sept-Dec 2020) via email through TTS. We requested completion by all Allied Health and Nursing professionals working within pediatric transplant, including both IPTA members and non-members.
Results:We received 119 responses from varying Allied Health and Nursing roles across the globe. Participants provided details regarding various components of their role, including clinical work, research, and teaching. More probing questions were also asked regarding possible barriers to providing optimal care and other areas of activity that practitioners would like to be involved in. In addition, participants also answered questions relating to how the COVID-19 pandemic had impacted clinical practice providing both positive (e.g., telehealth allowing for more equitable and accessible service provision, improved work-life balance, improved infection control) and negative (e.g., professional isolation, limited-service provision, and barriers to accessing telehealth services) consequences. Both qualitative and quantitative analysis of the results was completed.
Next Steps: The AHNP committee have submitted two abstracts to IPTA Prague 2022 and are currently preparing two manuscripts for submission to The Journal of Pediatric Transplantation entitled:- Allied Health and Nursing Practises in Pediatric Solid Organ Transplantation: An International Survey.
- Allied Health and Nursing Professionals in Pediatric Solid Organ Transplantation: Perceptions of COVID-19 and Impact on Roles, Practice, and Resource Allocation.
- The provision of AHNP-related education
i. Regular Webinars
Goals: To develop a series of joint TTS/IPTA webinars covering a range of relevant AHNP topics, drawing upon the expertise of members, and fostering relationships with other groups and societies. The following webinars have been hosted by AHNP Committee:- “Social Media Use in Pediatric Transplantation” - Presented in April 2020 and was well attended with over 40 delegates.
- “Tricks and Tips for Virtual Care in Pediatric Transplant” - Presented in November 2020 with 63 attendees registered.
- “The Impact of the COVID-19 Pandemic on Patient and Family Wellness” - Presented in April 2021 in collaboration with Pediatric Heart Transplant Society. This inaugural joint session was well attended with 125 attendees registered.
- Our fourth webinar is planned for Spring 2022 and will be focused on “Engaging Adolescents in Ongoing Transplant Care”
Webinar recording can be found on the IPTA website in the members only section:
Webinars (tts.org)
ii. Updates to the IPTA Website AHNP Committee page
Please check out our AHNP Profiles on the IPTA website.
To date, we have profiled the role of the Clinical Nurse Specialist, Dietitian, Psychologist and Pharmacist.
Click here
Please see the latest inclusion: Spotlight on Pharmacy: talking to a pediatric transplant pharmacist: her professional life, her challenges, her IPTA membership. Click the link below to read more:Click here
Our next profile will feature Dr. Caroline Piotrowski, Child Health Researcher.
Jenny Wichart & Anna Gold,
AHNP Committee Co-Chairs
Louise Bannister,
AHNP Committee Council Liaison
SPOTLIGHT:
Contemporary approaches to toxoplasmosis prevention: -
Dear IPTA members,
We are inviting you to participate in a Toxoplasmosis Survey evaluating prophylaxis strategies in pediatric solid organ transplant patients (heart, lung, liver, kidney, intestine) .
The survey should take 10 minutes to complete and is available at the following link:
We kindly ask you to complete it for your particular transplant population and share it with other pediatric transplant teams at your hospital.
We thank you in advance for your collaboration.
On behalf of IPTA ID Committee
Pediatric Transplantation
![]()
IMPACT FACTOR
The 2020 Impact Factors (IF) for Pediatric Transplantation (PETR) were released summer 2021: PETR saw another increase in the 2 year IF rising to 1.502 (up from 1.425) and the 5 yr IF increasing to 1.530 (up from 1.429). While we are exceptionally pleased at this steady improvement, the Editorial Board recognizes that to be considered highly competitive with authors we must continue to strive to increase this number. We thank all of our Editorial Board members and reviewers for their contributions to this effort!
EDITORIAL BOARD
Following our rejuvenation in 2019-2020, The Editorial Board of PETR continues to expand. We have added statistical support as well as radiology support to benefit our AEs and reviewers in assessing manuscript suitability for publication.
SPECIAL SECTIONS/ISSUES
PETR is very much interested in publishing Special Sections or Special Issues with a series of review articles on a specific overarching topic. In January we published the Special Issue on the topic “Healthy Living in Pediatric Transplant Patients” (Guest Editors Asha Moudgil and Priya Verghese). In July we published the “EBV/PTLD Consensus Conference manuscripts”. Presently our Special Issue Editors Stephen Marks and Jodi Smith are completing the work needed to publish another Special Issue on “Pediatric Organ Allocation”. We are aiming for this Special Issue to be published early 2022. If you have an idea on a Special Section/Issue of PETR on a cutting-edge topic that you would like to suggest, please contact the Editors-in-Chief Sharon Bartosh and Burkhard Tönshoff.
REVIEW ARTICLES
There is a ongoing initiative of the PETR Editorial Team on soliciting Review Articles for PETR from experts in the field. The Editors-in-Chief, the Deputy Editors and Associate Editors have identified several cutting-edge research topics or important clinical themes which require an update. Please contact us if you or your group is interested in joining us in this initiative.
SOCIAL MEDIA PLUS!
Thanks to Vikas R Dharnidharka, our Associate Editor for Social Media and Communications PETR continues to expand our social media presence thru Twitter. Additionally, we are adding Visual Abstracts to our journal publications! This will facilitate sharing of work on social media. Authors please remember to provide your Twitter handle, and whether you would be interested in participating in a Twitter journal club if your article is accepted.
Sharon M Bartosh and Burkhard Tönshoff
On behalf of Pediatric Transplantation
IPTA 2022


IPTA Fellows/AHNP Virtual Symposium
We recently had our first Virtual Fellows and Allied Health & Nursing Professionals Meeting. Please keep an eye out for the recordings on the IPTA website.
A separate 1 hour Q&A Session will be hosted on Friday 22nd October at 6pm ET. This was set up specifically for our colleagues who were unable to join due to time zone. To register, please click here:
Outreach Committee

The mission of the IPTA Outreach Committee is to facilitate access for children with end-stage organ failure to safe, ethical, and high quality solid organ transplantation worldwide, particularly in less medically developed areas. Outreach Committee tools to achieve this mission include the Outreach Program for support of individual centers as well as developing Outreach Projets with a broader scope.
The aim of the Outreach Program is to contribute to new pediatric transplant center development, but also to help existing centers seeking to expand their activity, or improve quality of transplant services. Currently, two projects in the field of pediatric kidney transplantation are being supported through the OC program : Bangalore, India (sponsoring center : Dallas, Texas) and Ibadan, Nigeria (Calgary, Alberta).
Information on the new Outreach Program will soon be available on the IPTA website, using the following link : https://www.tts.org/ipta-education/ipta-resources. The deadline for the 2022 Program is 30th April 2022. Please ensure that this information is transmitted to your « sister centers » abroad!
It is recommended to start applications as soon as possible, considering the documentation required, details of which will be shared on the IPTA website.
Beside the coming 2022 Outreach Program, OC is also working on several projects to be deployed during this 2021-2023 term, including :
- The organization of an Outreach Committee Workshop at the next 2022 IPTA Prague Congress. Several topics related to the development of pediatric transplantation worldwide will be discussed, including presentation of the Global Observatory of Donation and Transplantation, as well as of individual programs in Nigeria and Vietnam.
- The introduction of Digital Pathology, as a tool for development of (pediatric) transplantation worldwide
- The proposal to allow access to our journal Pediatric Transplantation for publications from « young » pediatric transplant programs in emerging countries.
Raymond Reding
Chair, Outreach Committee
Publication Committee

The main activities and tasks of the Publication Committee are related to three major pillars:
- Committee -driven projects: The Peer Mentoring program
- Collaboration with Pediatric Transplantation Editors
- IPTA quarterly Newsletter
The aim of this Committee is to focus on main topics related to pediatric transplantation for the entire transplant team, encouraging and providing tools for publication. The Publication Committee has started the Peer Mentoring Program at last IPTA meeting in Vancouver and has continued to work on it. The Peer Mentoring program has different mentoring levels aiming to assist younger IPTA members in improving writing skills and scientific output. By reaching out to the Education Committee, the program has been further developed through the SMARTER INITIATIVE. A webinar regarding Peer Mentoring program will be offered to the IPTA community.
Another committee project includes the assistance to Pediatric Transplant Editors in collection of definitions including content and methodological requirements for guidelines and statement manuscripts. The committee is continuously looking for cutting-edge topics that require an update and identifying colleagues who would like to get involved with these projects. The impact factor of Pediatric Transplantation Journal is now 1.63, compared to 1.425 in 2019.
The committee is also in charge of the quarterly member newsletter. Together with all chairs from other committees we try to come up with informative and lively newsletters that are appealing to IPTA members and non-members. The committee is open to suggestions on new topics to be added to the IPTA Newsletter. Please feel free to contact Marta L Monteverde:
Following the important suggestion of our current IPTA president, Carlos Esquivel, the Committee considers the importance of diversity in its daily work, balancing cultural confidence and competence, considering equity, diversity and inclusion in all initiatives moving forward. We aim to apply diversity to all writing and mentoring projects.
Marta L Monteverde
Chair, IPTA Publications Committee
A Literary Review from IPTA Education Committee

The COVID-19 pandemic has brought forth significant challenges in health-care delivery, especially regarding the use of telemedicine. Preventing unwanted exposures to high-risk populations such as the immunocompromised transplant patients in the safety of their homes while observing social distancing became imminent.1 However, effective and equitable healthcare requires standardized protocols, which was severely lacking for this new telehealth era. The development of telemedicine delivered through a HIPAA-compliant platform brought accessible and personable health care options to patients at home.2 The ability to access telemedicine platforms through mobile applications increased patient participation by removing technological barriers and enabled seamless virtual patient and provider interaction.
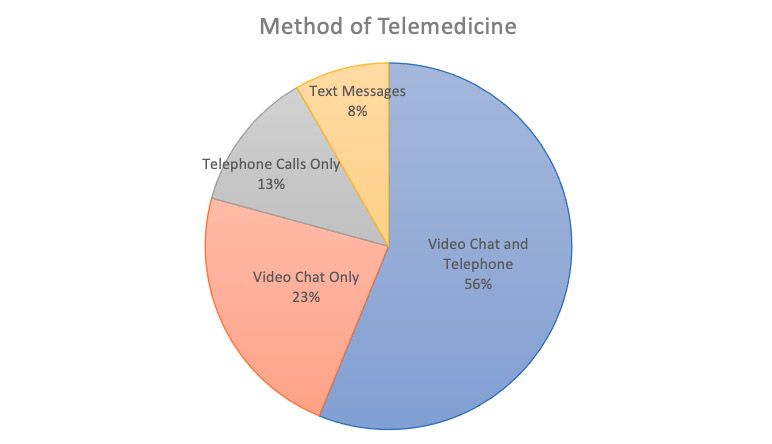
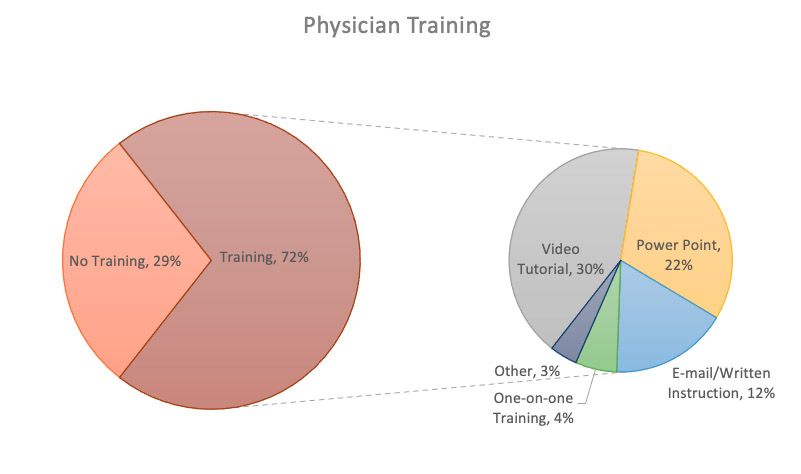
Telemedicine experiences during the pandemic can be summarized by Raina et al. which queried 197 pediatric nephrologists and 400 of their patients about their experiences. Figure 1 shows the preferred modalities for most physicians at 56% using both video chat and telephone calls, 23% using only video chat, 12.4% using only telephone calls, and 8.3% using only text messages. Physicians also used a wide variety of online systems to conduct synchronous telemedicine which included Zoom (23%), EPIC (9%), Doxy.me (7%), services not specified (37%), or a mix of local or smaller services (24%). Figure 2 highlights whether or not physicians received training (n = 141, 71%) in the use of telemedicine services as well as their method of training (42% video tutorial, 31% PowerPoint presentation, 17% e-mail and written instruction, 6% one-on-one training). Overall, the majority of physicians expressed satisfaction with the telemedicine experience with only 5% disappointed in the clinical aspect of telemedicine and only 4% disappointed overall. Most of their concerns were related to technological issues or the ability to view physical exams and/or laboratory results. In regards to the patient, most reported positive experiences as it was logistically easier and faster than in-person visits. Patients also felt that the quality of their visits were equal to what they would receive in person.3
Widespread acceptance of telemedicine services in fields such as pediatric nephrology emphasizes the need for the standardization of virtual care. A standardized workflow can potentially allow for more effective patient care, maintain clinical standards, but more importantly help ensure optimal patient outcomes with minimal risk of contracting COVID-19 or any potential infectious disease. Previous to the pandemic, emerging literature highlighted growing evidence of equal to above average clinical outcomes following the introduction of telemedicine in the postoperative setting. Complication rates were not statistically different between telehealth and traditional follow ups which ranged from 0-4.8% in procedures such as laparoscopic and open inguinal hernia repair, laparoscopic cholecystectomy, parathyroidectomy, arthroplasty, and pediatric urological procedures.4-8 As of now, no studies have reported statistically higher complication rates with telemedicine visits compared to traditional follow ups which supports its use in a wide array of specialties.9
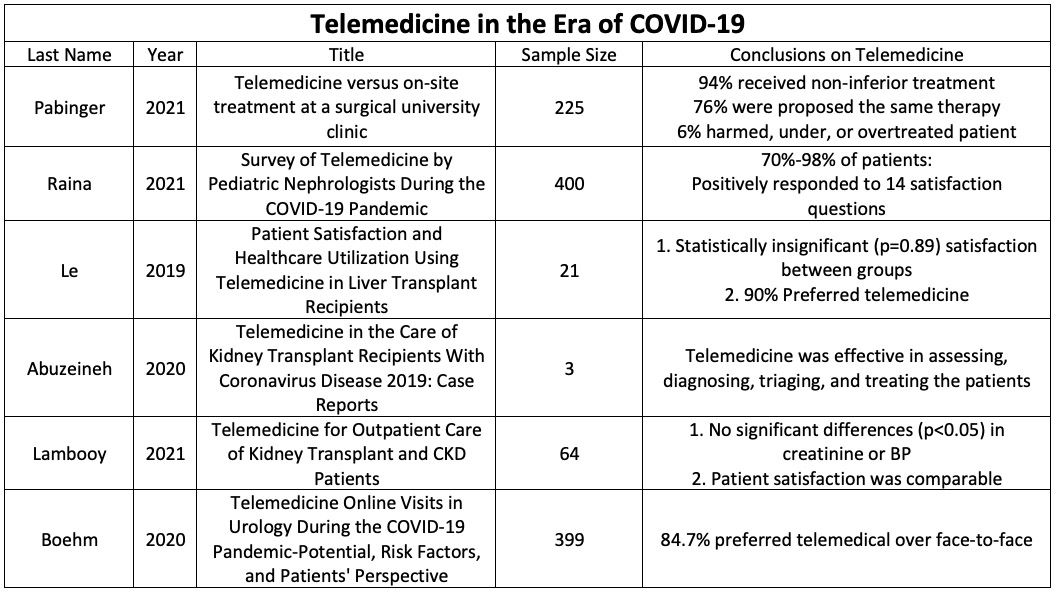
The University of Cincinnati Liver Transplant Program found that increasing posttransplant care between visits was a top priority for patients to improve function, quality of life, and independence.10 Technology and thereby telemedicine programs have the potential to personalize care to meet the needs of each individual patient. A small pilot study showed that developing a telemedicine-based home management program (THMP) was feasible and effective.10,11 Participants in this program had lower 90-day hospital readmission rates than the institutional and national averages (28% to 58%).12,13 Compared to their traditional follow up counterparts, individuals in the THMP program had significantly improved quality of life for physical function (p=0.02), social functioning (p=0.05), and general health (p=0.05).12,13 Patients noted that from their perspective, the biggest determinant for quality of life is time spent at home compared to the hospital. More importantly, there was no difference regarding health literacy assessments between the 2 groups as 90% of patients scored in the highest group, or ninth grade and above.14 In a similar cohort, Le et al. assessed whether telemedicine can be utilized to sustain strong patient-physician relationships in post-liver transplantation care and came to the same results and conclusion.15
Utilizing telemedicine to diagnose and triage patients has also shown great success in kidney transplant recipients, providing uninterrupted follow-up care to these high-risk individuals. Abuzeineh et al. followed three kidney transplant recipients with COVID-19 that were managed using telemedicine and found that this allowed transplant clinicians an expanded opportunity for patient questions, transmission of information, reassurance, and creating a sense of building a comprehensive care plan.16 By extension, this innovation could potentially help increase access to live kidney donor transplant evaluations, particularly important to those who have financial or transportation challenges.16 These concepts are reinforced by Wilkinson et al. which examined a similar situation in terminally ill cystic fibrosis patients awaiting transplantation.17 All of the telemedicine participants found that this modality made the patient feel more supported and less isolated to the cystic fibrosis hospital team, gave a sense of security in seeing their health care providers face to face, and made it convenient to discuss health issues. Compared to the control group, no differences were seen in quality of life, anxiety or depression, admission to the hospital, clinic attendance, or the use of intravenous antibiotics.17 More significantly, there was a positive correlation in the perception of body image for those in the telemedicine group compared to the control group after six months of interaction.
Pabinger et al. expanded on this ideology by evaluating if diagnosis and therapies of outpatients in general surgery can be assessed using a mobile healthcare communication app instead of personal contact. Out of 225 adult surgical outpatients, 84% of telemedical diagnosis matched the on-site diagnosis, 76% proposed the same therapy, and 94% did not receive any inferior treatment.18 In the remaining 6% of cases, the telemedical therapeutic regiment had the potential to harm, under, or over treat the patient.18 Despite a decreased waiting time and patient frequency, this fractional percentage emphasizes the potential dangers in completely dehumanizing healthcare consultations.
The pandemic stimulated the advancements of telemedicine in a healthcare system that is resistant to change. A standardized, secure, and HIPAA-compliant form of telemedicine has yet to be standardized, but even more concerning is the lack of standardized training (or lack thereof) for all physicians. Despite the widespread acceptance of, either due to fear of the pandemic or in order to opt for general convenience, the physician-patient relationship should not be taken for granted or lost in virtual technology. A number of pilot programs have opted to balance traditional and telehealth follow ups based on a case-by-case situation, however other primarily virtual programs threaten the longstanding respect and commitment individuals have for their healthcare providers. As the post-pandemic era continues to unfold, physicians and patients should work to honor and nurture that vital relationship whether it be in person or via telehealth.
Education Committee, Co-Chair
2. Carr BG and Hollander JE. Virtually perfect? Telemedicine for Covid-19. New Engl J Med 2020; 382: 1679–1681. 3. Concepcion BP and Forbes RC. Telemedicine in kidney transplantation. Kidney 2020; 360.
3. Raina R, Nair N, Yap HK, et al. Survey of Telemedicine by Pediatric Nephrologists During the COVID-19 Pandemic. Kidney Int Rep. 2021;6(9):2316-2322. Published 2021 Jul 7. doi:10.1016/j.ekir.2021.06.026
4. Hwa K, Wren SM. Telehealth follow-up in lieu of postoperative clinic visit for ambulatory surgery: results of a pilot program. JAMA Surg 2013;148:823-7. 10.1001/jamasurg.2013.2672
5. Canon S, Shera A, Patel A, et al. A pilot study of telemedicine for post-operative urological care in children. J Telemed Telecare 2014;20:427-30. 10.1177/1357633X14555610
6. Eisenberg D, Hwa K, Wren SM. Telephone follow-up by a midlevel provider after laparoscopic inguinal hernia repair instead of face-to-face clinic visit. JSLS 2015;19:e2014.00205
7. Sharareh B, Schwarzkopf R. Effectiveness of telemedical applications in postoperative follow-up after total joint arthroplasty. J Arthroplasty 2014;29:918-22.e1. 10.1016/j.arth.2013.09.019
8. Urquhart AC, Antoniotti NM, Berg RL. Telemedicine--an efficient and cost-effective approach in parathyroid surgery. Laryngoscope 2011;121:1422-5. 10.1002/lary.21812
9. Williams AM, Bhatti UF, Alam HB, Nikolian VC. The role of telemedicine in postoperative care. Mhealth. 2018;4:11. Published 2018 May 2. doi:10.21037/mhealth.2018.04.03
10. Ertel AE, Kaiser T, Shah SA. Using telehealth to enable patient-centered care for liver transplantation. JAMA Surg. 2015;150:674–675
11. Ertel AE, Kaiser TE, Abbott DE, et al. Use of video-based education and telehealth home monitoring after liver transplantation: results of a novel pilot study. Surgery. 2016;160:869–876.
12. Wilson GC, Hoehn RS, Ertel AE, et al. Variation by center and economic burden of readmissions after liver transplantation. Liver Transpl. 2015;21:953–960.
13. Paterno F, Wilson GC, Wima K, et al. Hospital utilization and consequences of readmissions after liver transplantation. Surgery. 2014;156:871–878.
14. Lee, Tiffany C.; Kaiser, Tiffany E.; Alloway, Rita; Woodle, Ervin Steve; Edwards, Michael J.; Shah, Shimul A. (2019). Telemedicine Based Remote Home Monitoring After Liver Transplantation. Annals of Surgery, 270(3), 564–572. doi:10.1097/sla.0000000000003425
15. Le LB, Rahal HK, Viramontes MR, Meneses KG, Dong TS, Saab S. Patient Satisfaction and Healthcare Utilization Using Telemedicine in Liver Transplant Recipients. Dig Dis Sci. 2019;64(5):1150-1157. doi:10.1007/s10620-018-5397-5
16. Abuzeineh, M.; Muzaale, A. D.; Crews,D.; et al. Telemedicine in the Care of Kidney Transplant Recipients with COVID-19: Case Reports. Transplantation Proceedings.2020; S0041134520326294–. doi:10.1016/j.transproceed.2020.07.009
17. Wilkinson, O. M; Duncan-Skingle, F.; Pryor, J. A; Hodson, M. E (2008). A feasibility study of home telemedicine for patients with cystic fibrosis awaiting transplantation. Journal of Telemedicine and Telecare, 14(4), 182–185. doi:10.1258/jtt.2008.070107
18. Pabinger C, Lothaller H, Lorenz A, Dammerer D. Telemedicine versus on-site treatment at a surgical university clinic: Study of 225 consecutive patients. Int J Med Inform. 2021;151:104460. doi:10.1016/j.ijmedinf.2021.104460
19. Lambooy S, Krishnasamy R, Pollock A, Hilder G, Gray NA. Telemedicine for Outpatient Care of Kidney Transplant and CKD Patients. Kidney Int Rep. 2021;6(5):1265-1272. Published 2021 Feb 26. doi:10.1016/j.ekir.2021.02.016
20. Boehm K, Ziewers S, Brandt MP, et al. Telemedicine Online Visits in Urology During the COVID-19 Pandemic-Potential, Risk Factors, and Patients' Perspective. Eur Urol. 2020;78(1):16-20. doi:10.1016/j.eururo.2020.04.055
Past Issues
IPTA Newsletters
- IPTA Newsletter - February 2026
- IPTA Newsletter - December 2025
- IPTA Newsletter - October 2025
- IPTA Newsletter - June 2025
- IPTA Newsletter - March 2025
- IPTA Newsletter - December 2024
- IPTA Newsletter - October 2024
- IPTA Newsletter - May 2024
- IPTA Newsletter - February 2024
- IPTA Newsletter - November 2023
- IPTA Newsletter - September 2023
- IPTA Newsletter - May 2023
- IPTA Newsletter - March 2023
- IPTA Newsletter - December 2022
- IPTA Newsletter - October 2022
- IPTA Newsletter - July 2022
- IPTA Newsletter - May 2022
- IPTA Newsletter - December 2021
- IPTA Newsletter - October 2021
- IPTA Newsletter - June 2021
- IPTA Newsletter - October 2020
- IPTA Newsletter - June 2020
- IPTA Newsletter - March 2020
- IPTA Newsletter - December 2019
- IPTA Newsletter - September 2019
- IPTA Newsletter - July 2019
- IPTA Newsletter - April 2019
- IPTA Newsletter - December 2018
- IPTA Newsletter - September 2018
- IPTA Newsletter - June 2018
- IPTA Newsletter - March 2018
- IPTA Newsletter - December 2017
- IPTA Newsletter - September 2017
- IPTA Newsletter - December 2016
- IPTA Newsletter - September 2016
Contact
Address
Cell Transplant and Regenerative Medicine Society
c/o The Transplantation Society
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada