


In the Northern Hemisphere we are in the middle of the Winter season, a season filled with holidays. There may be close to 20 holidays during this season. Some are celebrated worldwide and some regionally.
The reason I bring this up is that many of these holidays are celebrated indoors, and we are still facing the COVID-19 pandemic. As I am writing this letter, a new variant, Omicron, has been identified in 18 countries and is likely present in most others. However, it is too early to tell whether this variant is more transmissible than other variants, including Delta, or if it will cause more severe disease and whether the current vaccines and treatments will be less effective.
Do we need to be concerned? Yes, but I would say, very little! What we know is that the risk of transmission of COVID-19 is diminished if we follow all the precautions with which we have become accustomed: social distancing, mask-wearing, hand washing, and immunization.
Vaccines remain the most effective tool against COVID-19. We do need to protect our immunosuppressed children since most around the world are not or only partially vaccinated. I urge the manufacturers of the COVID-19 vaccine to make it available, particularly to low-resource countries. These countries remain vulnerable to continued disease and viral replication with almost no access to vaccines! The research for efficacy and safety in young children, particularly in immunocompromised kids, must be expedited, and I do hope pediatric transplant recipients will get priority when available.
Now, looking back, IPTA did have a very busy year. Here are some of the highlights:
- IPTA Fellows & Allied Health Symposium, October 2021
- SMARTER (Social Media for International Pediatric Transplantation) Initiative pioneered by the IPTA Education Committee (content has included a podcast, a Journal Club, and 2 webinars, more to come!)
- Launch of IPTA 2021 and 2022 Outreach Programs
- Endorsement of Declaration of Istanbul and development of Pediatric Priority position statement
- IPTA Allied Health & Nursing Professionals Committee webinar series
- Continuation of planning for IPTA 2022 Congress
In my humble opinion, I feel that we are coming out of this pandemic. I do wish the IPTA membership, and staff a Holiday Season filled with optimism, joy and love!
Yours faithfully,
Carlos O. Esquivel
IPTA President
IPTA Strategic Planning

Dear IPTA members,
We would like to announce an exciting new IPTA initiative of developing new guidelines across various organ systems as well as developing these in collaboration with other organizations, for publication in Pediatric Transplantation.
This is a call for:
- Volunteers – you may be early in your career and wish to learn how to develop guidelines, which can then be added to your CV; or you may be more advanced in your career but wishing to mentor more junior career colleagues.
- Your ideas! - Guideline topics ideas as well as suggestions of collaboration between different organizations would also be appreciated.
We ask you to send us your names and ideas by 10 January 2022. Please send to Katie Tait, IPTA Section Manager, at katie.tait@tts.org
Yours sincerely,
Mignon McCulloch
Past President, IPTA
Membership Committee

IPTA is over 500 members strong and the Membership Committee would like to thank current members for your continued engagement. We look forward to welcoming members to the 11th Congress of the International Pediatric Transplant Association in Prague, Czech Republic, where members will enjoy a reduced registration fee. In addition, IPTA members enjoy a number of benefits, including:
COVID-19 toolkit summarizing published SOT data with resource links for both IPTA members and SOT families:
COVID-19 Toolkit- Access to IPTA website, including Member’s Only section
- Subscription to Pediatric Transplantation
- Access to pediatric-related videos from TTS 2020
- Access to the IPTA quarterly newsletter
- Access to education from IPTA meetings including pediatric symposia from ATC and post-graduate course presentations
If you have already paid your 2022 dues, thank you for your support of IPTA! If you have not yet paid, please click here to renew your membership now. Your ongoing support is greatly appreciated!
Renew Your DuesSincerely,
Irene Kim
Chair, Membership Committee
Allied Health & Nursing Professionals Committee


We continue to spotlight our incredible Allied Health and Nursing Professionals Committee, this time focusing on Caroline Piotrowoski, Child Heath Researcher. Click below to read more about Caroline and her important work.
READ MOREIPTA 2022

If you haven’t registered for our in-person Congress in Prague in March 2022, please don’t forget to do so! Early Bird Registration ends on January 6th, 2022 so go ahead, give yourself a holiday treat and help children requiring transplant at the same time! For more information on our Meeting, including full Program and Registration, please click the link below.
Infectious Disease Committee
In our last IDCARE committee contribution to the IPTA newsletter, we provided a brief update on COVID-19 in pediatric solid organ transplantation (SOT) recipients. That was approximately 5 months into the pandemic – a time seemingly short and yet so long ago. We have learned much about the impact of SARS-CoV-2 in children and in SOT recipients in the interim, though knowledge gaps remain.1,2 It is only fitting that 1 year later, we now provide an update on SARS-CoV-2 and COVID-19 vaccines in children and in SOT recipients.
We now know that children can transmit and become infected with SARS-CoV-2.3-6 Indeed, the number of pediatric COVID-19 cases has increased since the start of the pandemic and as of early May 2021, children contribute to approximately 24% of all new COVID-19 cases in the US. The numbers for Europe and Latin America are currently unknown. Yet, these numbers are likely an under-representation of true COVID-19 burden in children, as it is estimated that > 22 million children in the US were likely infected.9 In general, COVID-19 causes milder disease and leads to fewer hospitalizations in children compared with adults.3,10-13 However, severe disease can occur and COVID-19 related pediatric deaths have now surpassed the highest recorded number of influenza-related deaths during the 2019-20 season in the US.8,14,15 Younger age and underlying comorbid conditions, including obesity, diabetes, and immunocompromise, have been identified as predictors of severe COVID-19 disease in children in some studies.16-20
When assessing COVID-19 data among SOT recipients, adult recipients are at risk for severe SARS-CoV-2 infection and in some studies have worse outcomes when compared with immunocompetent adults, with reported mortality rates of 13 to >30%.21-25 In addition, adult SOT recipients have been shown to have more rapidly waning immunity after natural infection compared with immunocompetent adults.26 Published data regarding acute COVID-19 among pediatric SOT recipients report a generally mild clinical course with outcomes similar to immunocompetent children.27,28 Similarly, the true burden of SARS-CoV-2 in pediatric SOT recipients is likely under-represented, including how the pandemic has affected pediatric transplantation.29-31 In addition, the emergence of multisystem inflammatory syndrome in children (MIS-C) or pediatric inflammatory multisystem syndrome (PIMS), suspected to be a post-infectious severe hyperinflammatory response to SARS-CoV-2 infection has been reported in a pediatric liver transplant recipient despite ongoing immunosuppression, that adversely affected the allograft.32
Global COVID-19 vaccination will be crucial in curbing the pandemic. Unfortunately, children and adult and pediatric SOT recipients were excluded from the initial COVID-19 vaccine trials. As medical advocates for our patients, we support and encourage their participation in COVID-19 vaccine clinical trials. Data are now emerging regarding the safety, immunogenicity, and efficacy of COVID-19 vaccines in adult SOT recipients. Extrapolating from experiences with other vaccines, it is expected that immunocompromised SOT recipients will have a blunted antibody response to COVID-19 vaccines. Indeed, preliminary data in adult SOT recipients report a lower percentage of patients mounting a positive antibody response after COVID-19 mRNA vaccines.33-35 In the largest series that included 658 SOT recipients, 54% of subjects had antibody detection a median of 29 days (28-31) after the second dose of COVID-19 mRNA vaccine and importantly, no alloreactivity was reported. These initial data were not poised to evaluate vaccine-induced cellular immunity or vaccine efficacy. Although the precise antibody correlate of SARS-CoV-2 protection remains to be established, durable vaccine-induced antibody concentrations have been reported to last 6 months after the second COVID-19 mRNA vaccine dose in immunocompetent individuals ≥ 18 years of age.36 Additional data are needed to evaluate the longevity of vaccine-induced antibody concentrations in the SOT population26 and future studies are expected to evaluate the need for possible booster vaccine doses.37 Additional data are also needed regarding efficacy of current COVID-19 vaccines against SARS-CoV-2 variants.38-40 Understanding these knowledge gaps may also help foster confidence in COVID-19 vaccination and reduce vaccine hesitancy.
Children represent ≥ 20% of the population in most countries, as such their inclusion in vaccine efforts may help contribute to achieving herd immunity. Data reported from COVID-19 mRNA vaccine clinical trials that enrolled immunocompetent children 12-15 years of age suggest that these vaccines are safe and effective in preventing COVID-19.
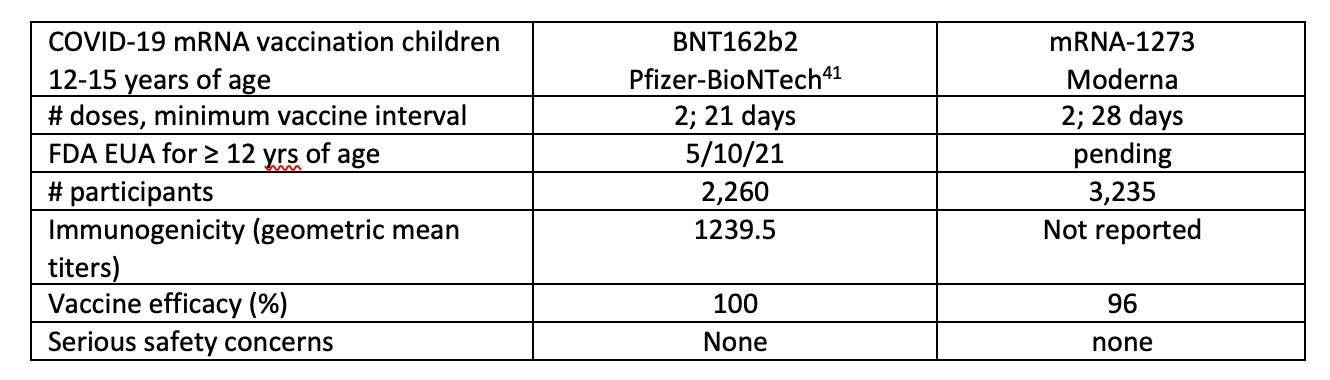
Indeed, the antibody response to the Pfizer vaccine in the 12 to 15-year-old age group was more robust than had been reported in the 16 to 25-year-old age group. Clinical trials in younger children are ongoing applying an age de-escalation strategy to evaluate vaccine safety and immunogenicity, with additional data expected for children 2-11 years old in the fall of 2021, followed thereafter in children 2 years to down to 6 months of age.
A similar post-vaccination side effect profile that was seen in adults has been reported in children 12-15 years, including fever, headache, fatigue, myalgias and arthralgias, occurring more frequently 24-48 hours after the second vaccine dose. In addition, children may develop localized reactive lymphadenopathy (neck, axillary) after vaccination. Severe reactions after COVID-19 mRNA vaccination are rare with anaphylaxis occurring in an estimated 2.5-11 cases per 1 million vaccine doses administered.42,43
Given the ongoing unknowns regarding the efficacy of COVID-19 vaccine in pediatric SOT recipients, immunocompromised patients may remain at risk for SARS-CoV-2 infection. As such, SOT candidates and recipients should continue to adhere to proven prevention strategies including wearing a properly fitted mask in children ≥ 2 years of age, practicing physical distancing, and performing good handwashing. It will be important to offer and encourage a cocoon strategy of protection by vaccinating household and close contacts of SOT recipients with COVID-19 vaccine when it becomes available to them.
Prepared by Monica Ardura, Arnaud G. L’Huillier, Michael Green, and Marian Michaels on behalf of the IPTA IDCARE committee
Ethics Committee
Case #1
A 5 year old child was diagnosed with focal segmental glomerulosclerosis. Her kidney function declined and she now requires hemodialysis. She had been doing well; however she was being considered for kidney transplantation. Her medical team recommended routine vaccination as a requirement for candidacy. Her family had agreed to only vaccinate against certain pathogens, but has refused vaccination against a newer virus in the community that is highly transmissible and for which there is an ongoing local epidemic. This virus has a high rate of causing partial paralysis in children from natural infection, has a 1% mortality rate, and is highly transmissible. The family refused vaccination because they are concern about safety and that it is a new vaccine. They stated that they will keep their child safe with masks and quarantining. However, the transplant team was unwilling to proceed with transplant and contacted child protective services to compel the vaccination.
Case #2
A 5 year old child was diagnosed with focal segmental glomerulosclerosis. Her kidney function declined and she now requires hemodialysis. She had been doing well; however she was being considered for kidney transplantation. Her medical team recommended routine vaccination as a requirement for candidacy. Her family had agreed to only vaccinate against certain pathogens, but has refused vaccination against a newer virus in the community that is highly transmissible and for which there is an ongoing local epidemic. This virus has a high rate of causing partial paralysis in children from natural infection, has a 1% mortality rate, and is highly transmissible. The family refused vaccination because they are concern about safety and that it is a new vaccine. They stated that they will keep their child safe with masks and quarantining. However, the transplant team was unwilling to proceed with transplant and contacted child protective services to compel the vaccination.
The prevalence of vaccine hesitancy and refusal has been increasing(1). Vaccination for transplant candidates is recommended prior to transplant and, often times on an accelerated time scale to help the child achieve immunity(2). However, despite these recommendations, not all recipients are up to date on age appropriate vaccinations. In addition, not all transplant programs are consistent in their policy of addressing vaccine refusal(3) . Should there be a policy of denial of transplant candidacy on basis of vaccine refusal? Nonmedical reasons for vaccine hesitancy have included philosophical or religious objections and personal beliefs that vaccines are unsafe and not necessary. Important questions remain. Is refusal to not vaccinate an indicator of non-adherence? Is non vaccination considered medical neglect? Does the acuity of the situation matter as in case #2 where the decision to list for transplantation had to be made quickly.
The principles of beneficence, autonomy, nonmaleficence and justice may provide framework to address these situations. Arguments to deny transplantation on basis of vaccine refusal include beneficence to the recipient as the vaccination will hopefully prevent disease, beneficence to others as preventing infection would protect others in the community, stewardship of protecting the organ from vaccine preventable complications as organs are a scarce resource. However, from a nonmaleficence e perspective, denying transplant would cause direct harm to the patient and in this case a child who may not have voice in these situations. From an autonomy perspective, vaccination may be considered medical coercion and affect a person’s autonomy and family trust with the medical team.
From a pediatric perspective, there is precedent for treatment over parental objections when children face serious immediate harm from parental decisions as in blood transfusion for children of Jehovah’s Witnesses(4). There is no legal precedent for requirement of routine vaccination of children over parental objections. Some states have viewed lack of vaccination as medical neglect but focus on parenteral education(5). However, if transplantation is important to survival of the child, and if it cannot be performed unless child is vaccinated and family refuses then transplant programs may need to re-consider these important issues. In such situations, a vaccination policy may be beneficial.
What are your thoughts on these cases? We would love to hear them! Please email Sections@tts.org with your responses, specifying which case you are referring to.
Prepared by Katheryn Gambetta and Tom Blydt-Hansen on behalf of the IPTA Ethics Committee
- Kates OS, Stohs EJ, Pergam SA, et al. The limits of refusal: An ethical review of solid organ transplantation and vaccine hesitancy. Am J Transplant. 2021;21(8):2637-2645. doi:10.1111/ajt.16472
- Danziger-Isakov L, Kumar D. Vaccination of solid organ transplant candidates and recipients: guidelines from the American society of transplantation infectious diseases community of practice. Clin Transplant. 2019; 33(9):e13563.
- Ladd JM, Karkazis K, Magnus D. Parental refusal of vaccination and transplantation listing decisions: a nationwide survey. Pediatr Transplant. 2013; 17(3): 244- 250
- Woolley S. Children of Jehovah's Witnesses and adolescent Jehovah's Witnesses: what are their rights? Arch Dis Child. 2005; 90(7): 715- 719.
- Parasidis E, Opel DJ. Parental refusal of childhood vaccines and medical neglect laws. Am J Public Health. 2017; 107(1): 68- 71

From all of us at IPTA, Happy Holidays, and we look forward to a healthy and prosperous 2022!
Past Issues
IPTA Newsletters
- IPTA Newsletter - February 2026
- IPTA Newsletter - December 2025
- IPTA Newsletter - October 2025
- IPTA Newsletter - June 2025
- IPTA Newsletter - March 2025
- IPTA Newsletter - December 2024
- IPTA Newsletter - October 2024
- IPTA Newsletter - May 2024
- IPTA Newsletter - February 2024
- IPTA Newsletter - November 2023
- IPTA Newsletter - September 2023
- IPTA Newsletter - May 2023
- IPTA Newsletter - March 2023
- IPTA Newsletter - December 2022
- IPTA Newsletter - October 2022
- IPTA Newsletter - July 2022
- IPTA Newsletter - May 2022
- IPTA Newsletter - December 2021
- IPTA Newsletter - October 2021
- IPTA Newsletter - June 2021
- IPTA Newsletter - October 2020
- IPTA Newsletter - June 2020
- IPTA Newsletter - March 2020
- IPTA Newsletter - December 2019
- IPTA Newsletter - September 2019
- IPTA Newsletter - July 2019
- IPTA Newsletter - April 2019
- IPTA Newsletter - December 2018
- IPTA Newsletter - September 2018
- IPTA Newsletter - June 2018
- IPTA Newsletter - March 2018
- IPTA Newsletter - December 2017
- IPTA Newsletter - September 2017
- IPTA Newsletter - December 2016
- IPTA Newsletter - September 2016
Social
Contact
Address
International Society of Uterus Transplantation
c/o The Transplantation Society
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada