


Dear IPTA Colleagues,
It has been a few weeks since our fantastic in-person meeting in Austin, and I hope this message finds you well. After a long Covid-induced break, we finally had the chance to reunite and enjoy a fantastic scientific program in a vibrant city. The IPTA council and committees had productive meetings to plan for IPTA's future in various ways. Thanks to Carlos Esquivel and Srinath Chinnakotla, as well as to Isabel Stengler, Catherin Parker and Katie Tait from TTS for making this unforgettable experience possible for us!
What will the next few years bring for IPTA? In the coming months, the IPTA committees will be renewed, with each one including a member who is a Fellow, as well as an Allied Health & Nursing Professional. A virtual Fellows and Allied Health & Nursing Professionals meeting is in the preliminary planning stages for 2024, and we would love to hear any ideas from IPTA members on this topic.
During our council meeting, we discussed how to involve more people in IPTA's daily work and to retain the knowledge of those who rotate off our committees. To achieve this goal, we plan to establish IPTA communities of experts step by step. The ID Care community will pilot this effort, and we will then discuss adding more communities that either mirror our committees or represent organs.
I am thrilled that Prof. Mignon McCulloch has agreed to stay on as the coordinator of our strategic planning process. She will support the coordination of our ideas in Outreach, Guidelines Development, Congress, Membership, Advocacy and other subjects that will be continuously developed further to secure the future of IPTA. We welcome any ideas and participation in this process from all IPTA members! Please don’t hesitate to contact our Section Manager Katie Tait (katie.tait@tts.org) if you like to engage yourself.
Lastly, I hope you all are enjoying the miracles of Springtime in the Northern Hemisphere, and the delights of Autumn down South!
Yours faithfully,
Lars Pape
IPTA President, 2023-2025

Report from the 12th Congress of the International Pediatric Transplant Association, Austin Texas 2023
The 12th Congress of the International Pediatric Transplant Association (IPTA) event in Austin, Texas, had over 400 attendees from 40 countries. The attendees included a diverse mix of pediatric transplant professionals from several specialties including pediatricians, surgeons, scientists, nurses, organ procurement personnel, advance transplant providers, pharmacists, administrators, fellows, residents, and students. The 4-day event featured nearly 200 abstracts, 90 oral presentations, 24 mini oral presentations, and more than 80 poster presentations. All of these presentations encouraged vibrant discussions and supported the exchange of new clinical and basic science information regarding clinical care management, basic science research, socioeconomic, and ethical and organ donation issues relevant to pediatric transplantation. We briefly describe here the highest scored presented abstracts at IPTA 2023 in clinical science.
Clinical Science
1.1 Liver Transplantation
Liver transplantation had a variety of topics that included organ allocation of pediatric livers for pediatric patients, normothermic perfusion, center volumes, and outcomes of pediatric liver transplantation for specific indications. A few papers were presented on allocation of pediatric livers. The group from NYU reported on the effect of acuity circle liver allocation policy on pediatric whole liver transplantation in high versus low volume centers and they noted that the median MELD/PELD decreased at both high volume and low volume centers with an increase in donor age.1 The second paper that was also well attended with robust discussion was presented by the Stanford group who examined the outcomes of pediatric liver transplant at high volume (>5 transplants per year) center versus low volume centers.2 Patients who travelled >100 miles to receive an out-of-state liver transplant at a high volume center had a better graft survival than patients who received a liver transplant at a local low volume center. There was no difference between the groups with respect to waitlist mortality and overall patient survival.2 The consensus was that more collaboration is required between transplant centers to exchange best practices to continue to improve access to care and outcomes for pediatric liver transplant recipients. New Zealand introduced a intention-to-split deceased organ livers in 2016, whereby all suitable organs from donors of 40 years and younger are split between a pediatric and adult recipient.3 The study presented from the University of Auckland group showed that the waitlist mortality had a downward trend (9.1 to 4.4%) and that the waitlist time was reduced for pediatric patients.3 The Dallas Children’s group reviewed 13 pediatric liver donors who had Normothermic perfusion in USA.4 The donors who received Normothermic perfusion were more likely to be DCD and have higher BMI. However, all the livers were transplanted into adult recipients and had excellent outcomes with no incidence of ischemic cholangiopathy in the DCD subgroup.4
Liver transplantation for pediatric patients with progressive familial intrahepatic cholestasis (PFIC) was reviewed by the Emory group and they noted that, unlike previous reports of hepatocellular carcinoma (HCC) occurring only in PIFC2, histologically proven HCC occurred in PFIC3 patients and recommended all patients with PFIC waiting for a liver transplant should be screened for HCC.5 The prevalence of portal vein obstruction from the Portal vein obstruction revascularization therapy after liver transplantation (PORTAL) registry from a 15 transplant centers collaborative was presented by Alfares et al.6 They noted that the overall prevalence of portal vein obstruction was 6.4% among all the patients and the highest prevalence (20%) was seen among biliary atresia recipients who were transplanted younger than one year of age using a living donor graft, and suggested that future studies should focus on prevention in this high-risk group.6 Bone Disorders are frequent in children undergoing liver transplantation. Astolfi et. al., presented a review of 105 children from Switzerland and they noted that 22 (21%) patients experienced pathological fractures.7 Patients with cholestatic liver disease and delay in bone age were at higher risk and they noted that nutritional intervention before liver transplantation cannot completely counteract the effect of chronic hepatic osteodystrophy due to liver disease and chronic cholestasis causing malabsorption.7 Pediatric living donor liver transplant patients sometimes develop graft fibrosis. Ueno et. al., presented 12 patients, where everolimus was initiated after a protocol biopsy showed graft fibrosis (METAVIR score >1) and they noted that graft fibrosis improved in 9 of the 12 patients at a median period of 33 months.8 Mouth ulcers were the significant side effects of everolimus resulting in discontinuation of the drug in one patient.8 Early extubation after liver transplant surgery has been demonstrated in pilot studies. Maudarbaccus et. al. presented 23/192 children over a 7-year period who were extubated in the operating room and none of them required reintubation in ICU.9 Preoperative and intra operative predictors of early extubation included older age, shorter length of surgery, smaller volume of PRBC and FFP transfused, and utilization of regional anesthesia. The early extubation group demonstrated a decreased ICU and hospital length of stay.9
1.2 Kidney Transplantation
The kidney transplantation had the highest number of abstracts (59) presented. There was a broad array of clinically interesting topics. Topics ranged from best practices for assessment for transplantation, use of cell free DNA, anti-body mediated rejection, and treatment of recurrent disease.
Adetunji et. al., from Cape Town, South Africa, reported on the use of Pediatric Feasibility Assessment for transplant, an objective and transparent system to assess the eligibility for transplantation to ensure consistency and equity in patient selection and to reduce moral distress among clinicians.10 Children who were not listed for transplant scored very low in social support adherence and caregiver concerns. Of note, the children who were not listed for transplant 46.7% (14/30) died within a year. This paper underscores the urgent need to implement psychosocial support to address remediable factors such as adherence, to address socio-economic barriers such as poverty, medical insurance, and to provide more comprehensive support for children awaiting renal transplantation in South Africa.10
Incidence, risk factors, treatment strategies, and outcome of antibody mediated rejection in the pediatric kidney transplant from the Cooperative European Pediatric Renal Transplant Initiative (CERTAIN) was presented by Fichtner et. al.,11 Data from 19 centers with 331 patients showed that the cumulative incidence of acute ABMR up to five years post-transplant was 10.8% and that of chronic ABMR was 5.9%. The risk factors for development of ABMR were the number of HLA-mismatches, evidence of de novo HLA-DSA, and T-cell mediated rejection.11 ABMR was a major risk factor for premature graft loss.11The group suggested standardization of treatment of ABMR and the need to develop novel drugs for more effective therapy of ABMR.
There were a few papers presented on the use of donor derived cell-free DNA. George et. al., used a composite risk factor of high donor cell-free DNA (>0.5%) combined with tacrolimus level variability that helped identify patients at increased risk for poor graft outcomes in the early post-transplant period.12
Pollack et. al., presented the use of Rituximab for PTLD prophylaxis in pediatric renal transplant patients with EBV viremia, which increased despite immunosuppression reduction. Rituximab was effective for EBV clearance and well tolerated.13
Kadakia et. al., presented the use of Belatacept based immunosuppression for (n=18) patients, where the primary indication conversion was rejection and/or noncompliance or calcineurin toxicity.14 Median time to conversion was 37 months, 94% (17/18) of the patients were compliant with monthly infusions and had fewer rejections after conversion, and GFR was preserved in 72% (13/18) of the patients and the authors report that Belatacept is an effective option for pediatric kidney transplant patient with nonadherence.14
1.3 Heart and Lung Transplantation
Pediatric heart transplant has been performed for childhood cancer patients with end stage heart failure and most centers required two years wait time after chemotherapy completion. Gambetta et. al., presented their series of five patients who received heart transplants less than two years prior to chemotherapy completion; median time to completion of chemotherapy was six months in the study.15 Cancer diagnosis included acute lymphoblastic leukemia and osteosarcoma. All patients are alive at a median follow up of 15 years.15 The authors suggest that select patients may do well with less than the traditional two years wait time. Adolescent thoracic transplant recipients are at increased risk of psychological distress and Liang et. al., presented an iPeer2Peer Program that encouraged confidence and disease self-management in 14 thoracic organ transplant recipients.16 Delvia et. al., evaluated functional performance in 16 children after lung transplant and they noted significant limitations in physical fitness in the pediatric lung transplant recipients even at one year post transplant and emphasized the need for rehabilitation with focus on strength and endurance training to optimize recovery from lung transplantation to improve long term health in this population.17
- Kim J, Ishaque T, Stern J et al.
Effects of acuity circle liver allocation policy on pediatric whole liver transplants in high versus low volume transplant centers. Pediatr Transplant 2023; 27:3 (s) e14477. https://doi.org/10.111/petr.14477 - Bozhilov K, Stotlz D, Bonham A et al.
Pediatric Liver Transplant at a Long-Distance high volume centers confers improved graft survival compared to local low volume transplant centers. Pediatr Transplant 2023; 27:36 (s) e14477. https://doi.org/10.111/petr.14477 - Evans H, Mouat S, McCall J et al.
Reduction of waiting time and waiting list mortality for pediatric liver transplantation following introduction of an intention to split allocation policy. Pediatr Transplant 2023; 27:39 (s) e14477. https://doi.org/10.111/petr.14477 - Sanchez-Vivaldi J, Kadakia Y, MacConmara M et al.
Utilization of normothermic machine perfusion in pediatric donor livers. Pediatr Transplant 2023; 27:61 (s) e14477. https://doi.org/10.111/petr.14477 - Cimeno A, Lo D, Soler-Rodriguez D et al.
Liver transplantation in pediatric patients with progressive familial intra hepatic cholestasis: A large single center experience with recommendations for malignancy screening. Pediatr Transplant 2023; 27:5 (s) e14477. https://doi.org/10.111/petr.14477 - Alfares B, Bokkers RPH, de Kleine RHJ et al.
Prevalence of portal vein obstruction in pediatric patients after liver transplantation; a multicenter, observational, prevalence study. Pediatr Transplant 2023; 27:3 (s) e14477. https://doi.org/10.111/petr.14477 - Astolfi D, Rock N, Mclin VA et al.
Predictors for pathological bone fractures in children undergoing liver transplantation. . Pediatr Transplant 2023; 27:4 (s) e14477. https://doi.org/10.111/petr.14477 - Ueno T, Takase K, Deguchi K et al.
Impact of everolimus treatment for graft fibrosis based on pathological findings after pediatric living donor liver transplantation. Pediatr Transplant 2023; 27:34 (s) e14477. https://doi.org/10.111/petr.14477 - Maudarbaccus MF, Siddiqui A
Predictors of early extubation after pediatric liver transplant. Pediatr Transplant 2023; 27:114 (s) e14477. https://doi.org/10.111/petr.14477 - Adetunji A, Gajjar P, Luyckx V et al.
Evaluation and the implementation of a pediatric feasibility assessment for transplantation (pFAT) form in children and adolescents at Red Cross War Memorial Children’s Hospital (RCWMCH) CapeTown, SA Pediatr Transplant 2023; 27:23 (s) e14477. https://doi.org/10.111/petr.14477 - Fichtner A, Gauche L, Hoecker B et al.
Incidence, risk factors treatment strategies and outcome of antibody-mediated rejection in pediatric kidney transplant recipients-a multicenter analysis of the Cooperative European Pediatric Renal Transplant Initiative (CERTAIN). Pediatr Transplant 2023; 27:14 (s) e14477. https://doi.org/10.111/petr.14477 - George R, Aeckersberg G, Hitchman K et al.
Utility of donor-derived cell free DNA and tacrolimus variability in monitoring early post-kidney transplant outcomes. Pediatr Transplant 2023; 27:42 (s) e14477. https://doi.org/10.111/petr.14477 - Pollack S, Eisenstein I, Plonsky M et al.
Rituximab for PTLD prophylaxis in pediatric renal transplant recipients. Pediatr Transplant 2023; 27:60 (s) e14477. https://doi.org/10.111/petr.14477 - Kadakia Y, Vivaldi JS, McConnell L et al.
Belatacept-based immunosuppression in pediatric kidney transplantation. Pediatr Transplant 2023; 27:88 (s) e14477. https://doi.org/10.111/petr.14477 - Gambeta K, Morgan E.
Timing is everything:Single center’s experience of early heart transplantation for Anthracycline Cardiotoxicity. Pediatr Transplant 2023; 27:12 (s) e14477. https://doi.org/10.111/petr.14477 - Liang M, Lin J, Siqueria I et al.
“it made me feel like I wasn’t alone”. The experience and perspectives of adolescent thoracic transplant recipients participating in the iPeer2Peer support mentorship program. Pediatr Transplant 2023; 27:12 (s) e14477. https://doi.org/10.111/petr.14477 - Deliva R, Grasemann H, Solomon M et al.
Functional performance and fitness in pediatric lung transplant candidates and recipients: a retrospective review. Pediatr Transplant 2023; 27:14 (s) e14477. https://doi.org/10.111/petr.14477

Patient Voices - Madelyn’s Story
As part of the Opening Ceremony at the IPTA Congress in Austin, pediatric transplant recipients and their parents shared their experiences and journeys. We thought you might enjoy reading this story about 9 year old Madelyn Quinn, a heart transplant recipient in the USA, who was recently interviewed on the Gayle King show on CBS News. Please click on the link below to see Madelyn’s inspiring and heart-warming story as she continues on her transplant journey.

Literary Review
Solid organ transplantation (SOT) is a multi-faceted discipline of medicine that relies on the correspondence of surgical and medical staff in the pre- and post- operative management of critically ill patients with end organ dysfunction. The process begins far prior to surgery with the screening of patients that suffice as surgical candidates and the identification of a tissue match. Patients spend weeks to months with medical management alone while they await a surgical resolution to their end organ dysfunction. Once suitable tissue is obtained, SOT involves a complex surgical procedure with dissection of an organ from a donor and implantation into recipient. Intricate anti-rejection medical management is then pursued to ensure the continued functionality of the recipient’s new organ. Anti-rejection therapy is aggressive and requires close follow up for appropriate titration of the regimen to ensure functionality while limiting undesirable side effects, most notably severe immunocompromising effects.
In Spring of 2020, the COVID-19 pandemic emerged and significantly impacted the discipline of SOT, changing management in this population of patients considerably. The effects of COVID-19 on SOT were thoroughly examined in the recently published comprehensive review: The effects of COVID-19 on pediatric and adult solid organ transplant recipients and the emergence of telehealth. This comprehensive review aimed to summarize, analyze, and update data on the clinical course of COVID-19 in SOT activities. Additionally, the review also utilized global data to highlight the advantages and disadvantages of the emergence of telehealth in SOT care. Comprehension of new data is imperative to adequately weigh the risks and benefits of performing transplants during and after the pandemic and to analyze telehealth as a viable modality to deliver care for post-operative follow-up visits.
Initially, the most noticeable impact of COVID-19 on SOT management was a drastic decrease in the number of organ donors and transplantation procedures. The cause of a decrease in SOT procedures is multifactorial; however, it can be directly correlated to limited hospital capacity, reduced availability of medical personnel, and a general decrease in operative load attributed to pandemic burden.
Additionally, concerns for virus transmission cannot be ignored. Anti-rejection therapy creates an immunocompromised state and monumentally increases the risk of viral transmission in solid organ transplant recipients (SOTR). SOTR are also at increased risk of amplified severity of symptoms and complications related to infection. Increased symptom burden in SOTR has led to further development of new treatment approaches including monoclonal antibodies and convalescent plasma to treat or prevent infection.
Furthermore, SOTR patients require comprehensive post-operative management for anti-rejection care which creates a need for office visits, increasing the opportunity for viral transmission. In response to these concerns, transplant centers adapted their post-transplant care protocols to include virtual consultations with focus on remote monitoring and titration to medical regimens.
The emergence of telehealth in SOT care during the pandemic presented the opportunity to examine its direct effects on quality of care. Thirteen studies analyzed by the comprehensive review focused on the delivery of post-transplant care by telehealth; and these studies suggest increased medical adherence, higher satisfaction rates, and increased ability to obtain measurements. Patient surveys examined show patients appeared satisfied with the level of privacy during the consultation and with the quality of professional patient health care.
Although these factors support telehealth as an efficient means of healthcare delivery for post-transplant care several drawbacks do exist. Most notably these drawbacks include the challenge of carrying out a complete objective physical examination and repercussions of poor connection with reduced audio and/or image quality. Additional hurdles include the reliability of connectivity, need for high-speed internet, legal and ethical issues, data security, and patient confidentiality, all of which can decrease effective and timely use of telehealth.
COVID-19 has changed the practice of SOT and has provided the medical field with the opportunity to evaluate potential areas of improvement in the management of SOTR.
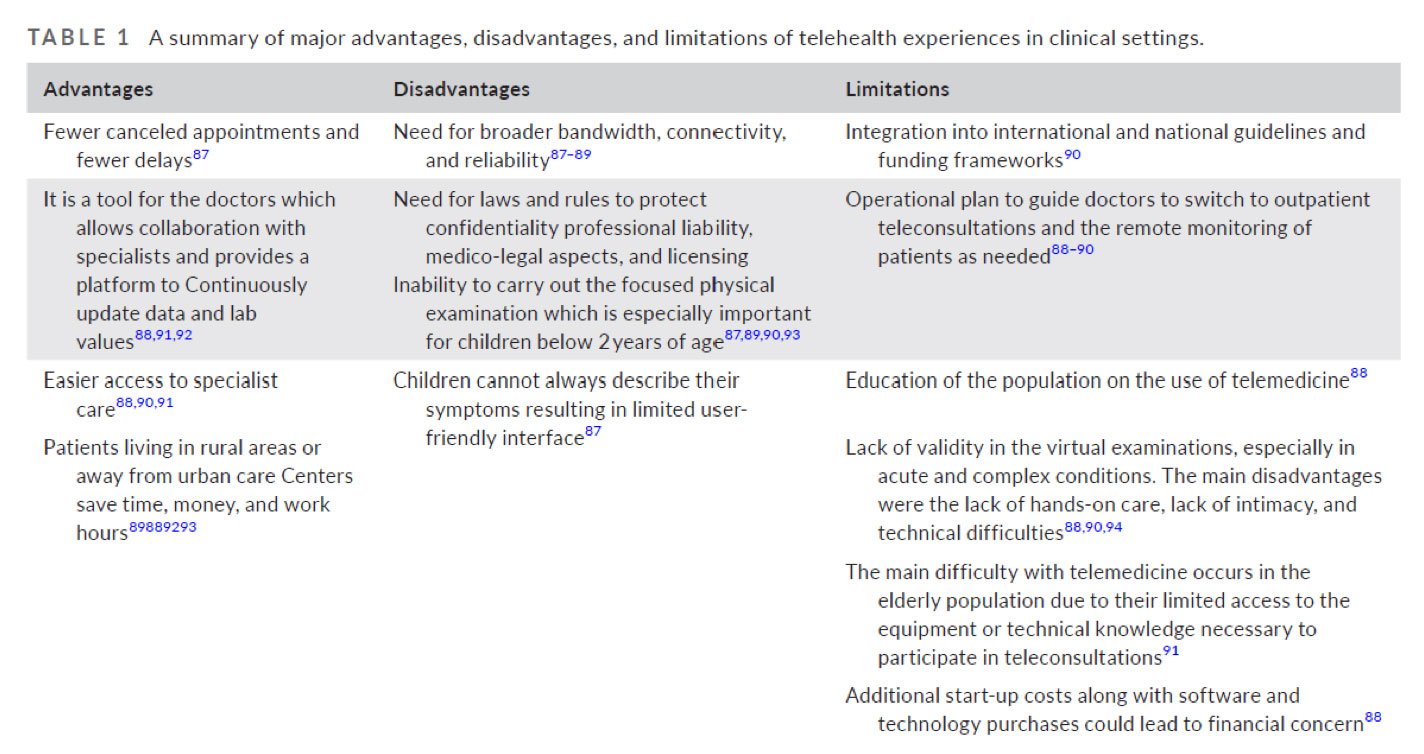
Table 1: adopted from The effects of COVID-19 on pediatric and adult solid organ transplant recipients and the emergence of telehealth1
- Raina R, Shah R, Marks SD, Johnson JN, Nied M, Bhatt GC, Bonham CA, Datla N, Sethi SK, Bartosh SM.
The effects of COVID-19 on pediatric and adult solid organ transplant recipients and the emergence of telehealth. Pediatr Transplant. 2023 Mar 6:e14490. doi: 10.1111/petr.14490. Epub ahead of print. PMID: 36879358.

Update
The IPTA Membership Communications Committee is delighted to report that IPTA membership is currently at an ALL-TIME HIGH of 920 members!
The merging of the Membership and Communications Committees in 2021 brought together the passion for growing IPTA inherent within the Membership Committee with the dedication to sharing IPTA’s message embodied by the Communications Committee.
Developments spearheaded by the combined Membership Communication Committee include the setting up of IPTA’s Social media platforms as well as IPTA’s own dedicated ListServ. Being able to communicate in real-time across channels has resulted in increased dialogue with members and would-be members, particularly around important events such as the 12th IPTA Congress in Austin, Texas, in March 2023. If you haven’t already, please follow IPTA on Twitter on www.twitter.com/IptaPedsTx, and join the IPTA ListServ www.tts.org/ipta-members-area/ipta-listserv
For both this Congress and the previous Virtual Congress in March 2022, a combination package of Congress Registration including 1 years IPTA Membership was offered. For both Congresses, this initiative was a resounding success which resulted in a significant uptake in IPTA membership (an increase of 305 new members in 2022 and then a further increase of 116 new members in 2023), particularly amongst Emerging Economies and Trainees - 2 core areas of membership which IPTA is particularly keen to drive.
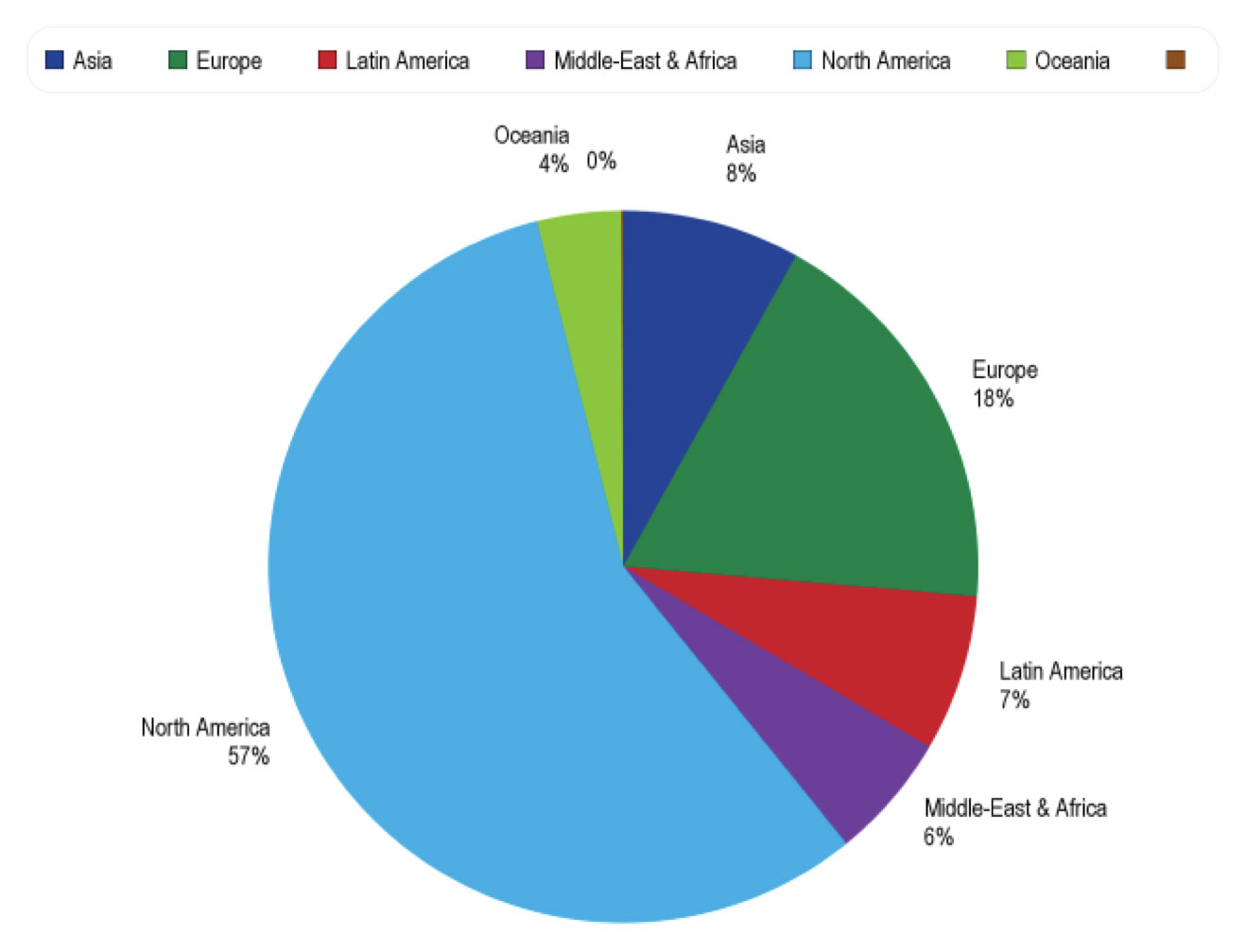
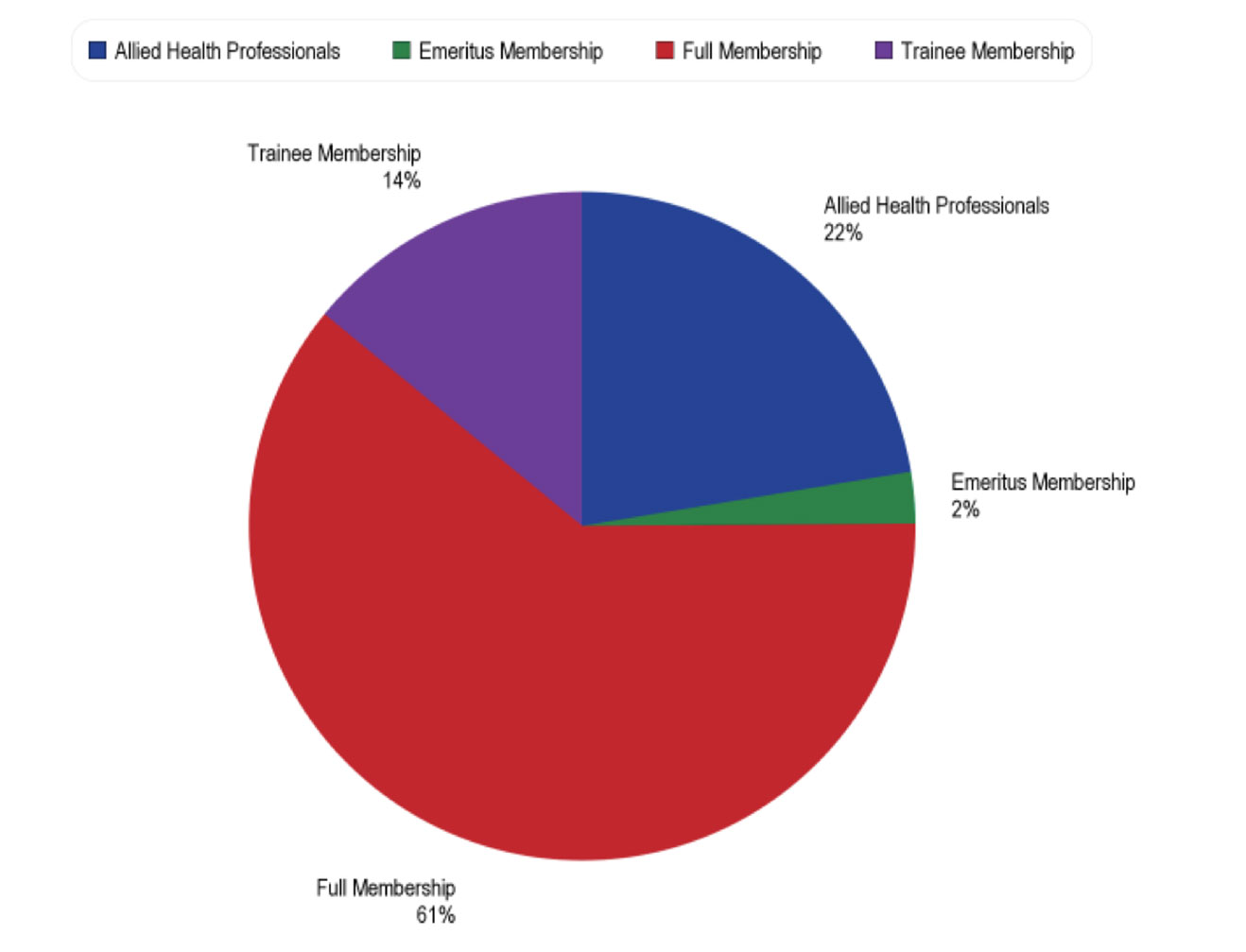
As you can see from the graphics below, IPTA membership is now truly global, spanning 6 continents, with an increasing number of Trainees and Allied Health & Nursing Professionals becoming part of the Society.
Membership by Region
Membership by Membership Type
Spread the word! If you know someone who you feel should become an IPTA member, please share this link www.tts.org/ipta-members-area/ipta-join or ask them to email sections@tts.org
Let’s keep up this momentum and grow the Society to 1000+ members!

Infectious Diseases CARE (Clinical care, Advocacy, Research, and Education) Committee
In our last two IDCARE committee contributions to the IPTA newsletter, we focused on COVID-19 in pediatric solid organ transplantation. Clearly, now three years later we have moved into a new phase of the COVID-19 pandemic, but an update is still appropriate. Fortunately, COVID-19 causes milder disease and leads to fewer hospitalizations in children compared with adults even for our vulnerable immunosuppressed transplant patients. But we should not be cavalier as they are still at greater risk for disease than their immunocompetent compatriots. Particularly, during the current time when many countries, schools and hospitals are relaxing masking policies it is important for us to remember lessons learned from the earlier periods of the pandemic. We must remain vigilant. We must continue to promote immunization, as vaccines, available for children 6 months of age and over, remain one of our best preventive strategies against severe infection. Accordingly, we should emphasize the importance of COVID-19 immunization for our candidates, recipients, close contacts, and all health care personnel. In addition, transplant centers and our families should be cognizant of local COVID-19 activity levels. Our patients can consider masking and maintain social distancing during periods increased immunosuppression or if the COVID-19 incidence increases in their community.
This year, however, we want to give some updates that are not COVID-19 related.
First off, transplant teams should be aware that some of the common community viruses such as respiratory syncytial virus and influenza are still appearing at unusual times. Invariably these viruses will impact our pediatric SOT recipients as well and we need to remain vigilant about patterns of circulation occurring with atypical seasonality.
Second, we want to inform the community of some achievements and ideas for the future.
It was so wonderful to see everyone at IPTA 2023 in Austin and to be able to resume our face-to-face community interaction. We were excited by the number of presentations and degree of involvement in the meeting by the ID community.
A round of applause and deep gratitude goes out to colleagues Steve Webber, Upton Allen, and Michael Green for leading the Herculean task of producing the IPTA post transplant lymphoproliferative disease (PTLD) consensus guidelines. Publications of several are already available and we anticipate the rest being submitted for publication this summer [1, 2]. This successful endeavor involved 28 IPTA colleagues from 8 countries and was a truly momentous and rewarding effort. This collaborative, multidisciplinary effort and the involvement of participants from across the globe highlights the strengths of our IPTA community.
As noted above, collaboration and multidisciplinary engagement are key aspects of IPTA. As such, we are very excited to announce that ID CARE will be the first IPTA committee to pilot a model for expanded IPTA member engagement in our activities and efforts. The IPTA Council approached us about this concept at the Austin meeting and we were enthusiastic about its possibilities. Through this new large interest group structure, we eagerly welcome all IPTA members with interest in advocacy, research, and/or education related to prevention and treatment of infectious diseases that impact pediatric transplantation. We look forward to engaging with many across varying levels of expertise and emphasize that this desire for broadened engagement is not limited to infectious disease physicians. Our mission has always been to promote an international network of professionals dedicated to the prevention and management of infections in pediatric transplantation recipients. The proposed larger group will allow for greater involvement of the IPTA community in the development and leadership of ID related projects with the oversight of a small leadership committee. We believe that this innovation will further invigorate the already highly productive IDCARE committee and provide a framework for future application of this model to other IPTA committees and working groups. Stay tuned as we put the finishing touches on this plan and be on the lookout for IPTA announcement to sign up for community of ID experts.
Meanwhile, stay healthy, wash your hands, and vaccinate!
- Wilkinson JD, Allen U, Green M et al.
The IPTA Nashville consensus conference on post-transplant lymphoproliferative disorders after solid organ transplantation in children: I-Methodology for the development of consensus practice guidelines. Pediatr Transplant 2022; e14333. DOI: 10.1111/petr.14333 - Green M, Squires JE, Chinnock RE et al.
The IPTA Nashville consensus conference on Post-Transplant lymphoproliferative disorders after solid organ transplantation in children: II-consensus guidelines for prevention. Pediatr Transplant 2022; e14350. DOI: 10.1111/petr.14350

Now Accepting Applications!
We are delighted to announce that applications for the 2023 Outreach Program are now open.
The mission of the IPTA Outreach Committee is to facilitate access for children with end-stage organ failure to safe, ethical, and high-quality solid organ transplantation worldwide, particularly in less medically developed areas. Outreach Committee tools to achieve this mission include the Outreach Program for support of individual centers, as well as developing Outreach Projects with a broader scope.
The aim of the Outreach Program is to contribute to new pediatric transplant center development, but also to help existing centers seeking to expand their activity, or improve quality of transplant services.
Currently, two projects in the field of pediatric kidney transplantation are being supported through the OC program: Cali, Colombia (sponsoring center: Toronto, Canada) and Lviv, Ukraine (sponsoring center: Brussels, Belgium). Funding for further projects is available in 2023.
If your center is interested in participating, please take a look at the information available on the IPTA website. Click the link below to visit the 2023 Outreach Program page.
The deadline for the 2023 Program is July 31, 2023. Please ensure that this information is transmitted to your sister centers abroad!
Please do not hesitate to reach out to Katie Tait, IPTA Section Manager, at katie.tait@tts.org if you have any questions.
In the meantime, we will look forward to receiving your applications!

Nonadherence & Graft Dysfunction
The IPTA Ethics Committee would like to assess how the transplant community views nonadherence, especially if re-transplantation is required.
We are conducting a survey to better understand how pediatric transplant professionals approach this problem across the world to help prevent and provide some guidance.
We would appreciate your participation and time.

SAVE THE DATE
IPTA 2025!

Past Issues
IPTA Newsletters
- IPTA Newsletter - February 2026
- IPTA Newsletter - December 2025
- IPTA Newsletter - October 2025
- IPTA Newsletter - June 2025
- IPTA Newsletter - March 2025
- IPTA Newsletter - December 2024
- IPTA Newsletter - October 2024
- IPTA Newsletter - May 2024
- IPTA Newsletter - February 2024
- IPTA Newsletter - November 2023
- IPTA Newsletter - September 2023
- IPTA Newsletter - May 2023
- IPTA Newsletter - March 2023
- IPTA Newsletter - December 2022
- IPTA Newsletter - October 2022
- IPTA Newsletter - July 2022
- IPTA Newsletter - May 2022
- IPTA Newsletter - December 2021
- IPTA Newsletter - October 2021
- IPTA Newsletter - June 2021
- IPTA Newsletter - October 2020
- IPTA Newsletter - June 2020
- IPTA Newsletter - March 2020
- IPTA Newsletter - December 2019
- IPTA Newsletter - September 2019
- IPTA Newsletter - July 2019
- IPTA Newsletter - April 2019
- IPTA Newsletter - December 2018
- IPTA Newsletter - September 2018
- IPTA Newsletter - June 2018
- IPTA Newsletter - March 2018
- IPTA Newsletter - December 2017
- IPTA Newsletter - September 2017
- IPTA Newsletter - December 2016
- IPTA Newsletter - September 2016
Social
Contact
Address
International Society of Uterus Transplantation
c/o The Transplantation Society
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada