



Presidential Message

Dear Friends & Colleagues,
I am honored and humbled to be carrying the baton as President of this superb international organization that advocates for children with organ transplantation.
One of my first rotations as an intern was in Pediatrics. I strongly considered to pursue this specialty, but I knew I wanted to become a surgeon. Years later, I ended up at the University of Pittsburgh, starting a fellowship in transplantation. I was not totally convinced I wanted to become a transplant surgeon, let alone a pediatric transplant surgeon. Within a few weeks into the fellowship, my mentor, Tom Starzl, said something that surprised me, and that was: “Carlos, I need you to take care of the pediatric patients”! That was the beginning of an amazing journey that paved the way to my involvement with IPTA. IPTA is a multidisciplinary association that mimics the work we do on a daily basis, and hence, our work is the foundation of this organization. At least, this is the way I see it!
The evolution of pediatric transplantation has improved immensely in terms of patient and graft survival; however, we continue to face many ongoing problems such as mortality on the waiting list because of scarcity of organs, side effects of immunosuppressive medications, and long term attrition from non-adherence to treatment, but the biggest problem is lack of access to health before and/or after transplantation. The COVID-19 pandemic has exacerbated the socioeconomic disparity in healthcare.
To that end, one of my priorities as President is to enhance dissemination of already existent educational programs in the organization and to create novel ones by using digital platforms, expanding upon our existing SMARTER initiative of webinars, podcasts and Journal Clubs. Another key priority for me is to recruit members from countries where they need us the most.
The mission of this Society is primarily about education and sharing knowledge. I think that in the last decade some countries were so remote and isolated, but now everyone has a smart phone. I think we are going to reach every single corner of the world. As mentioned before, IPTA, with its very active committees, is very well positioned to make a difference for so many children who suffer from organ failure or from complications around transplantation. It is important to increase the presence of IPTA worldwide (particularly to geographic areas with large population of children living below the poverty line). I envision IPTA developing partnerships with local societies and academic institutions. The financial health of the organization may be improved from grants from foundations as well as from individual philanthropic donations.
I would like to make you aware that IPTA will host a Virtual Meeting for Fellows and Allied Health & Nursing Professionals on October 14th and 15th 2021. This meeting is free to IPTA and TTS members. Please keep a look out for more news in the upcoming months, but put the date in your diaries for now.
I would also like to remind you about our upcoming Congress in Prague on March 26-29th 2022, where we look forward to welcoming you all in-person.
Please see https://ipta2022.org/ for more information, and to submit an abstract!
I would like to extend a very warm welcome to our new Councillors and Committee members. I look forward to our work together. To the continuing Councillors and Committee members, thank you for your ongoing commitment to IPTA. To our outgoing Councillors and Committee members, thank you for your tremendous hard work and dedication.
Best wishes,
Carlos O. Esquivel
IPTA President
Literary Review

Examination of Donor Allocation in Pediatric Heart Transplantation
The waitlist mortality for children awaiting heart transplantation approaches 20-30% worldwide1,2. Despite this, 40% of all potential donor organs are not used1. These organs may be declined by transplant centers for many reasons, including perceived poor donor quality, specific preferences of transplant teams (cardiologists and surgeons), local or national regulations, distance, or considerations depending on the match for recipient size and blood type. There are also marked differences internationally in the local availability of heart transplantation, with many countries not having access to pediatric heart transplant centers or care. Regulatory concerns are paramount in transplant clinicians’ minds – in a recent survey by Godown et al, survey respondents indicated that recent transplant program mortalities and concern for regulatory restrictions on transplant programs affected which organs they accepted3.
Several publications have recently attempted to find a consensus on what constitutes an “acceptable” donor heart. Richard Kirk, Anne Dipchand and colleagues brought together 62 authors within the International Society of Heart and Lung Transplantation (ISHLT) to examine this issue and come up with a consensus statement1. While the primary document was published in ISHLT’s journal, the series of papers looking at the seven different components of this consensus were published in IPTA’s journal, Pediatric Transplantation4-11. These papers included many members of IPTA, as well as several speakers in the upcoming 11th IPTA Congress in Prague who will be discussing several of these topics across all organ systems.
Despite a rigorous literature review, it was clear in these articles that there is not enough available evidence to make clear recommendations about many of the addressed issues. From a pure medical assessment of donor “health”, the single most important parameter was the function of the donor heart; as long as this was normal, little else affected outcomes.
Intriguingly, the impact of decision-making skills and behavioral economics was brought to the forefront in this series of articles4. A series of biases were identified by a team of behavioral psychologists that can affect the donor acceptance rates, including incentive bias, omission and outcome biases, and overall risk aversion. Further, even the way the information about donors is presented (including whether other centers with higher priority on the list have already declined) could affect how a clinician decides about a potential donor. Regulatory reporting was an important factor as well, with examples given in the Butler et al paper showing how a more selective transplant program could “appear” to have better survival despite their overall patient survival (if one included waitlist survival) being lower than other programs.
The impact of potential biases on donor acceptance clearly needs further consideration and research by our transplant community. These biases should be considered by regulatory bodies when adjudicating transplant performance, with oversight systems modified to promote donor utilization and patient survival from the time of listing.
ReferencesMembership Committee

Dear IPTA Colleagues,
We remain very grateful for and reliant upon members’ ongoing support. Thank you to those who have renewed their membership for 2021! We continue to have a significant proportion of our members who have not yet renewed, and our committee is actively reaching out to engage with unpaid members individually. We strongly encourage all members to renew IPTA membership today, not only to take advantage of the many benefits but also to continue to support IPTA programs.
IPTA members enjoy a number of benefits, including:
- COVID-19 toolkit summarizing published SOT data with resource links for both IPTA members and SOT families
- Access to IPTA website, including Member’s Only section
- Subscription to Pediatric Transplantation
- Access to pediatric-related videos from TTS 2020
- Access to IPTA quarterly newsletter
- Reduced registration fees for biennial Congress with upcoming Congress in Prague 2022
Access to education from IPTA meetings including pediatric symposia from ATC and post-graduate course presentations
If you have already paid your 2021 dues, thank you for your support of IPTA!
If you have not yet paid,
to renew your membership now. Your ongoing support is greatly appreciated!
Sincerely,
Chair, Membership Committee
Meet the Greats!


Dr Elisabeth Hodson
Emeritus Pediatric Nephrologist Sydney, Australia
Elisabeth is a pediatric nephrologist who trained at London Hospital Medical College in medicine/pediatrics. She came to Australia from the UK in 1975. She subsequently spent 8 months at the University of Minneapolis, Minnesota learning about dialysis and transplantation in children with Professor Michael Mauer. She received her FRACP in 1979 and was appointed staff specialist at the Children’s Hospital in Sydney.
In 1982 she married Dr Tom Karplus and with him spent three years working in pediatric haematology-oncology at the University of California, San Diego followed by the Scripps Clinic in La Jolla, California. Her work, which is the most cited, focused on antibodies to the glycoprotein IIB/IIIA receptor on platelets, and these antiplatelet agents are used during percutaneous coronary angioplasty with or without stents. After returning to Australia in 1985, Elisabeth was appointed in pediatric nephrology at the Children’s Hospital at Camperdown and at Prince of Wales Children’s Hospital in Randwick. In 1989 Elisabeth moved to join the Pediatric Department at Westmead Hospital in Sydney as a pediatric nephrologist and set up dialysis and transplantation for children at Westmead Hospital.
In 1994, she took over as Head of Pediatrics at Westmead Hospital, and in 1995 she amalgamated the Pediatric Service at Westmead Hospital with the New Children’s Hospital at Westmead. In the new hospital she led efforts to set up hemodialysis and hemofiltration services and kidney transplantation for children. Elisabeth remained head of Nephrology until 2008. In 2005 Elisabeth became Co-Chair for the Medical Programme and remained in that role until her retirement in 2010. Elisabeth led the Cochrane Renal Group systematic reviews on nephrotic syndrome in children.
Since then she has written or supported the writing of 21 Cochrane systematic reviews. Elisabeth has been involved in formulating KDIGO guidelines on nephrotic syndrome and IPNA guidelines on steroid resistant nephrotic syndrome in children. Since 2002 Elisabeth has led the Antecedents of Renal Disease in Aboriginal Children and Young People Study and she continued her involvement in this study until 2020.
She has led the training of pediatric nephrologists around the world and has been instrumental in the support of pediatric kidney transplantation across Australia and New Zealand for over 30 years.
LEADERS IN ALLIED HEALTH & NURSING

Beverly Kosmach-Park, DNP, RN, FAAN
Clinical Assistant Professor of Surgery Clinical Nurse Specialist, Liver and Intestine Transplant Department of Transplant Surgery Children’s Hospital of PittsburghBeverly is the Clinical Nurse Specialist for the Abdominal Transplant Department at Children’s Hospital of Pittsburgh. She works with patients and families throughout the transplant process from evaluation for transplant to transition to adult care. Beverly has spoken internationally on transplant-related topics in pediatric liver and intestine transplantation and transition of care and has authored several articles, book chapters, and nursing and patient educational materials. She has been an active member of IPTA since 2013. She has served as Co-Chair of the Allied Health Providers Committee (2017-19) and participated in the Scientific Planning Committee and AHP Planning Committees for the international symposia in 2017 and 2019. She received the IPTA Outstanding AHP Award in 2019.
Beverly is also active within the American Society of Transplantation (AST) and has served on the Executive Committee for the Pediatric Community of Practice. Within that group, she chaired a task force that designed a transition toolkit template for transplant centers and helped launch the Transition Portal. Beverly was on the Board of Directors of the International Transplant Nurses Society (ITNS) for 9 years, serving as President and Education Director. She has chaired and co-chaired numerous transplant conferences and symposia and has been active in program planning for these meetings, including ITNS, AST, IPTA, and the Pediatric Intestinal Failure and Rehabilitation Symposium. Beverly was inducted as a Fellow in the American Academy of Nursing (FAAN) in 2013.
She has been the Director of Camp Chihopi, a summer camping event for children who are liver or intestine transplant recipients, since 1995. Developing a virtual version of Camp Chihopi during the pandemic was challenging but proved to be very successful and enjoyed by all! Although Chihopi will again be virtual this summer, she is hopeful the campers and staff will be together again in 2022.
IDCARE Committee
Children, Solid Organ Transplantation, and SARS-CoV-2
In our last IDCARE committee contribution to the IPTA newsletter, we provided a brief update on COVID-19 in pediatric solid organ transplantation (SOT) recipients. That was approximately 5 months into the pandemic – a time seemingly short and yet so long ago. We have learned much about the impact of SARS-CoV-2 in children and in SOT recipients in the interim, though knowledge gaps remain.1,2 It is only fitting that 1 year later, we now provide an update on SARS-CoV-2 and COVID-19 vaccines in children and in SOT recipients.
We now know that children can transmit and become infected with SARS-CoV-2.3-6 Indeed, the number of pediatric COVID-19 cases has increased since the start of the pandemic and as of early May 2021, children contribute to approximately 24% of all new COVID-19 cases in the US.7,8 Yet, these numbers are likely an under-representation of true COVID-19 burden in children; for example, it is estimated that > 22 million children in the US were likely infected.9 In general, COVID-19 causes milder disease and leads to fewer hospitalizations in children compared with adults.3,10-13 However, severe disease can occur and COVID-19 related pediatric deaths have now surpassed the highest recorded number of influenza-related deaths during the 2019-20 season in the US.8,14,15 Younger age and underlying comorbid conditions, including obesity, diabetes and immunocompromise have been identified as predictors of severe COVID-19 disease in children in some studies.16-20
Assessment of COVID-19 data among SOT recipients demonstrates that adult recipients are at risk for severe SARS-CoV-2 infection, with some studies showing SOT recipients to have worse outcomes compared with immunocompetent adults, with reported mortality rates of 13 to >30%.21-25 In addition, adult SOT recipients have been shown to have more rapidly waning immunity after natural infection compared with immunocompetent adults.26 Published data regarding acute COVID-19 among pediatric SOT recipients report a generally mild clinical course with outcomes similar to immunocompetent children.27,28 However, the true burden of SARS-CoV-2 in pediatric SOT recipients is likely under-represented , including the pandemic’s impact on a broad array of pediatric transplant-related issues.29-31 In addition, the emergence of multisystem inflammatory syndrome in children (MIS-C) or pediatric inflammatory multisystem syndrome (PIMS), suspected to be a post-infectious severe hyperinflammatory response to SARS-CoV-2 infection, raises additional concerns for pediatric SOT recipients. MIS-C has been reported in a pediatric liver transplant recipient despite ongoing immunosuppression and had an adverse impact on the allograft.32
Global COVID-19 vaccination will be crucial in curbing the pandemic. Children and immunocompromised individuals, including SOT recipients, were excluded from the initial COVID-19 vaccine trials. As medical advocates for our patients, we support and encourage the participation and inclusion of children and SOT recipients in COVID-19 vaccine clinical trials. Data are now emerging regarding the safety, immunogenicity, and efficacy of COVID-19 vaccines in adult SOT recipients. Extrapolating from experiences with other vaccines, it is expected that immunocompromised SOT recipients will have a blunted antibody response to COVID-19 vaccines. Indeed, preliminary data in some adult SOT recipients report a lower percentage of patients mounting a positive antibody response after COVID-19 mRNA vaccines.33-36 In the largest series that included 658 SOT recipients, 54% of subjects had antibody detection a median of 29 days (28-31) after the second dose of COVID-19 mRNA vaccine and importantly, no alloreactivity was reported.36 Younger adults and liver transplant recipients had improved vaccine response compared to other subjects. These initial data were not poised to evaluate vaccine-induced cellular immunity or vaccine efficacy. Although the precise antibody correlate of SARS-CoV-2 protection remains to be established, durable vaccine-induced antibody concentrations have been reported to last 6 months after the second COVID-19 mRNA vaccine dose in immunocompetent individuals ≥ 18 years of age.37 Additional data are needed to evaluate the longevity of vaccine-induced antibody concentrations in the SOT population26,38 and future studies are expected to evaluate the need for possible booster vaccine doses.39 Likewise, data are also needed regarding efficacy of current COVID-19 vaccines against SARS-CoV-2 variants.40-43 Understanding these knowledge gaps may also help foster confidence in COVID-19 vaccination and reduce vaccine hesitancy.
Children represent ≥ 20% of the population in most countries, as such their inclusion in vaccine efforts may help contribute to achieving herd immunity. Data reported from COVID-19 mRNA vaccine clinical trials that enrolled immunocompetent children 12-15 years of age suggest that these vaccines are safe and effective in preventing COVID-19.
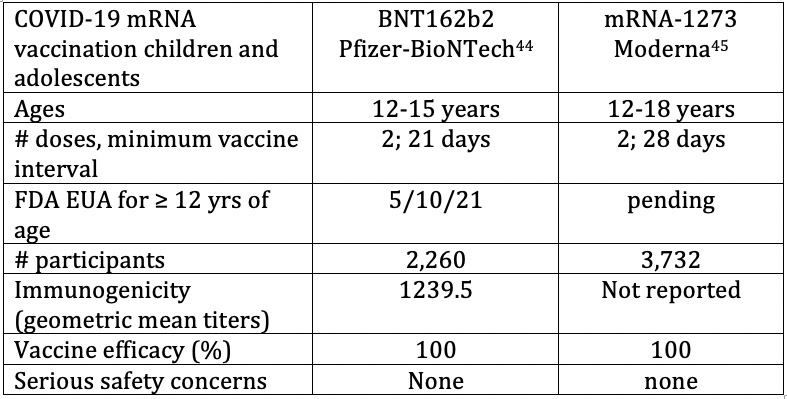
Notably, the antibody response to the Pfizer vaccine in the 12 to 15-year-old age group was more robust than had been reported in the 16 to 25-year-old age group. Clinical trials in younger children applying age de-escalation and dose escalation strategies to evaluate vaccine immunogenicity and safety are currently ongoing. Additional data are expected for children 2-11 years old in the fall of 2021, followed thereafter in children down to 6 months of age.
A similar post-vaccination side effect profile that was seen in adults has been reported in children 12-15 years, including fever, headache, fatigue, myalgias and arthralgias, occurring more frequently 24-48 hours after the second vaccine dose. In addition, children may develop localized reactive lymphadenopathy (neck, axillary) after vaccination. Severe reactions after COVID-19 mRNA vaccination are rare with anaphylaxis occurring in an estimated 2.5-11 cases per 1 million vaccine doses administered.46,47
We strongly encourage SOT candidates and recipients 12 years of age and older to be vaccinated. Given the ongoing unknowns regarding the efficacy of COVID-19 vaccine in pediatric SOT recipients and until more of the population is vaccinated, immunocompromised patients may remain at risk for SARS-CoV-2 infection. As such, SOT candidates and recipients should continue to adhere to proven prevention strategies including wearing a properly fitted mask in children ≥ 2 years of age, practicing physical distancing when in large groups or indoors, and performing good handwashing. It will be important to offer and encourage a cocoon strategy of protection by vaccinating household and close contacts of SOT recipients with COVID-19 vaccine when it becomes available to them.
and Marian Michaels on behalf of the IPTA IDCARE committee
IPTA COUNCIL 2021-2023
We welcome our new Council!
IPTA COMMITTEES 2021-2023
The following Committees have welcomed new members. Please see below for more information.
P
A new call for Committee members will go out in Spring 2022. Watch this space for more information and how to apply!
Please click here
and click on each Committee.
IPTA 2022


Past Issues
IPTA Newsletters
- IPTA Newsletter - June 2026
- IPTA Newsletter - February 2026
- IPTA Newsletter - December 2025
- IPTA Newsletter - October 2025
- IPTA Newsletter - June 2025
- IPTA Newsletter - March 2025
- IPTA Newsletter - December 2024
- IPTA Newsletter - October 2024
- IPTA Newsletter - May 2024
- IPTA Newsletter - February 2024
- IPTA Newsletter - November 2023
- IPTA Newsletter - September 2023
- IPTA Newsletter - May 2023
- IPTA Newsletter - March 2023
- IPTA Newsletter - December 2022
- IPTA Newsletter - October 2022
- IPTA Newsletter - July 2022
- IPTA Newsletter - May 2022
- IPTA Newsletter - December 2021
- IPTA Newsletter - October 2021
- IPTA Newsletter - June 2021
- IPTA Newsletter - October 2020
- IPTA Newsletter - June 2020
- IPTA Newsletter - March 2020
- IPTA Newsletter - December 2019
- IPTA Newsletter - September 2019
- IPTA Newsletter - July 2019
- IPTA Newsletter - April 2019
- IPTA Newsletter - December 2018
- IPTA Newsletter - September 2018
- IPTA Newsletter - June 2018
- IPTA Newsletter - March 2018
- IPTA Newsletter - December 2017
- IPTA Newsletter - September 2017
- IPTA Newsletter - December 2016
- IPTA Newsletter - September 2016
Contact
Address
International Pediatric Transplant Association
c/o The Transplantation Society
740 Notre-Dame Ouest
Suite 1245
Montréal, QC, H3C 3X6
Canada